By Sridevi R. Pitta, MD, MBA; Rahul Sharma, MD; Konstantinos Dean Boudoulas, MD
Introduction
Transradial access (TRA) is widely used for percutaneous coronary intervention (PCI) procedures due to its association with lower bleeding and vascular complications compared to transfemoral artery access. However, post-procedural radial artery occlusion (RAO) remains a common and significant complication, which can restrict future use of the same radial artery for procedures and as a conduit for coronary artery bypass graft.
The incidence of RAO following coronary angiography has varied from less than 1% to up to 33% in early studies, but contemporary practice shows a lower incidence of around 4.6%.2 Despite this, RAO is often underdiagnosed as most patients remain asymptomatic due to collateral arterial perfusion. Further analyses have identified female sex, larger sheath size, and lower body mass index as potential risk factors for RAO.2 Various techniques have been described to prevent RAO, such as patent hemostasis protocols and prophylactic ipsilateral ulnar compression. Preventive strategies for RAO following TRA procedures are crucial to minimizing complications and ensuring the success of future interventions, starting from access to hemostasis .1,2,3,4,5 Below are some key strategies.
Interventional Approaches
Newer access methods for radial artery cardiac catheterization have been developed to reduce complications and improve patient outcomes.
- Ultrasound-guided radial access: This method involves using real-time ultrasound to guide the cannulation of the radial artery, which facilitates successful sheath placement during catheterization procedures. The use of ultrasound guidance has been shown to reduce the time to TRA, improve the first-pass attempt, and reduce the total number of attempts. Minimizing repeat radial artery needle punctures helps decrease arterial wall trauma, which is a significant factor in preventing RAO (Figures 1A and 1B).
- Distal radial artery access: This method is considered a safe and effective alternative for conducting coronary procedures and can be routinely used in all patients, depending on the operator’s experience. The use of distal radial artery access has been shown to reduce the incidence of RAO compared to traditional methods since it overlies the carpal bones, which allows for quicker hemostasis and also allows maintenance of antegrade flow to the hand by the superficial palmar arch branch (Figure 2).
- Radial artery-to-sheath: A ratio of less than 1 was identified as an independent predictor for postprocedural occlusion of the radial artery. Women receiving a 7 French sheath had an incidence of radial occlusion of 25%. Therefore, aiming for smaller sheath sizes and pre-interventional sizing of the radial artery for sheath size selection might be potential approaches to reduce this vascular complication and ensure the success of future interventions.4
- Pharmacologic strategies: RAO prevention includes the intraprocedural administration of anticoagulant agents. Both intra-arterial and intravenous unfractionated heparin (UFH) are equally effective in preventing RAO, based on randomized data. The SPIRIT OF ARTEMIS study confirmed that high-dose UFH is more effective than standard-dose UFH in preventing RAO following diagnostic coronary angiography with radial access. In this multi-center study, 1,836 patients were randomized to receive either high-dose UFH (100 IU/kg body weight) or standard-dose UFH (50 IU/kg body weight). The results showed that the rate of RAO was significantly lower in the high-dose UFH group compared to the standard-dose group (3.0% vs. 8.1%; p < 0.001), with no significant increase in bleeding complications.7 Prevention of a radial artery spasm with the use of intra-arterial nitroglycerin or nondihydropyridine calcium channel blockers, such as verapamil, lowers the incidence of RAO.8
Hemostasis Methods
Various techniques have been described to prevent RAO.
- Patent hemostasis protocols: This technique involves applying just enough pressure to prevent bleeding through the vascular puncture without causing complete collapse of the vessel under pressure. This method helps maintain blood flow and reduces the risk of RAO.
- Ipsilateral ulnar compression: This technique significantly lowers the risk of RAO after TRA coronary intervention. In a trial of 3,000 patients undergoing diagnostic cardiac catheterization, the 30-day incidence of RAO was 0.9% among those randomized to prophylactic ipsilateral ulnar compression and standard hemostasis and 3.0% among patients treated with standard hemostasis alone. This technique is considered effective, safe, and inexpensive. Standardized radial compression procedures and other potential approaches for prevention of radial occlusion include more careful application of hemostasis techniques.9
- Hemostatic patch protocols: In the STAT 2 trial, potassium ferrate hemostatic patch (PFHP) as an adjunct to the TR Band (TRB) facilitated an early deflation. It showed time to complete TRB deflation was significantly shorter with the PFHP (66 ± 14 minutes) compared to the TRB alone (113 ± 56 minutes) (P < 0.001). Minor rebleeding requiring TRB reinflation was much more frequent without the PFHP (0% vs. 67.7%; P < 0.001), with 2.3 ± 1.3 additional reinflation and deflation attempts needed for hemostasis. Hematomas developed in 4.0% of the PFHP group and 6.8% of the TRB group (P = 0.20).2 RAO was rare (<1%), although 41% of patients received <5,000 U heparin.2 Among PCI patients, time to TRB deflation (68 ± 15 minutes vs 138 ± 62 minutes; P < 0.001) and composite complications (10.0% vs. 24.2%; P = 0.04) were reduced with the PFHP.2 Compared with the TRB alone, the PFHP facilitated early 60-minute TRB deflation following transradial catheterization, with a numeric reduction in vascular complications. RAO occurs rarely with early deflation regardless of heparin dose (Figures 3A and 3B)10
Conclusion
RAO remains a significant complication following transradial catheterization, but various strategies must be utilized, starting from access to hemostasis, which are crucial to minimizing complications and ensuring the success of future interventions
References
- Bernat I, Aminian A, Pancholy S, et al. Best Practices for the Prevention of Radial Artery Occlusion After Transradial Diagnostic Angiography and Intervention. An International Consensus Paper. JACC Cardiovasc Interv. 2019 Nov 25;12(22):2235-2246.
- Didagelos M, Afendoulis D, Pagiantza A, et al. Treatment of radial artery occlusion after transradial coronary catheterization: a review of the literature and proposed treatment algorithm. Hellenic J. Cardiol. 2025 Feb 3:S1109-9666(25)00008-9.
- Tsigkas G, Papanikolaou A, Apostolos A, et al. Preventing and Managing Radial Artery Occlusion following Transradial Procedures: Strategies and Considerations. J. Cardiovasc. Dev. Dis. 2023 Jun 30;10(7):283.
- Schlosser J, Herrmann L, Böhme T, et al. Incidence and predictors of radial artery occlusion following transradial coronary angiography: the proRadial trial. Clin Res Cardiol. 2023 Sep;112(9):1175-1185.
- Hadjivassiliou A, Kiemeneij F, Nathan S, et al. Ultrasound-guided access to the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: a technical guide. EuroIntervention. 2021 Mar 19;16(16):1342-1348.
- Seto AH, Roberts JS, Abu-Fadel MS, et al. Real-time ultrasound guidance facilitates transradial access: RAUST (Radial Artery access with Ultrasound Trial). JACC Cardiovasc Interv. 2015 Feb;8(2):283-291.
- Hahalis GN, Leopoulou M, Tsigkas G, et al. Multicenter Randomized Evaluation of High Versus Standard Heparin Dose on Incident Radial Arterial Occlusion After Transradial Coronary Angiography: The SPIRIT OF ARTEMIS Study. JAAC Cardiovasc Interv. 2018 Nov 26;11(22):2241-2250.
- Abdelazeem B, AT Mohamed , ASVolgman et al. The efficacy of nitroglycerin to prevent radial artery spasm and occlusion during and after transradial catheterization: A systematic review and meta-analysis of randomized controlled trials Clinical Cardiology 2022
- Pancholy SB, Bernat I, Bertrand OF, et al. Prevention of Radial Artery Occlusion After Transradial Catheterization: The PROPHET-II Randomized Trial. JACC Cardiovasc Interv. 2016 Oct 10;9(19):1992-1999.
- Safirstein JG, David MT, Schussler JM, et al. Radial Hemostasis Is Facilitated With a Potassium Ferrate Hemostatic Patch: The STAT2 Trial. JACC Cardiovasc Interv. 2022 Apr 25;15(8):810-819.
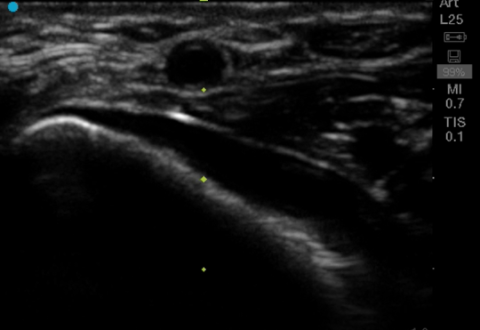
Figure 1A: Ultrasound- guided proximal radial artery access.
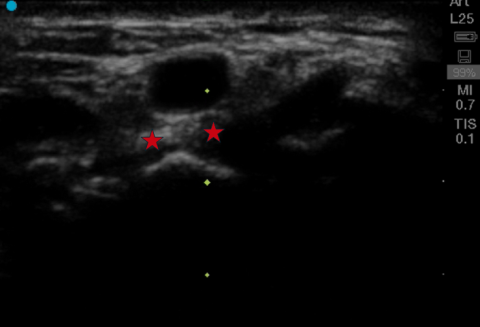
Figure1B: Ultrasound-guided distal radial artery access that overlies the carpal bones. (asterisk)
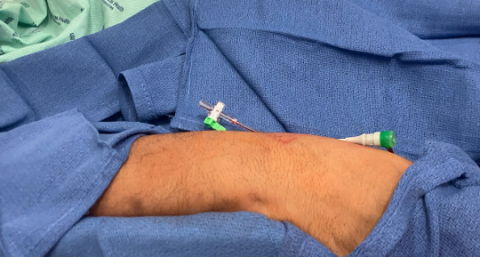
Figure 2: Distal radial artery access and positioning

Figure 3A: Utilization of hemostasis patch, along with TRB (stat seal).
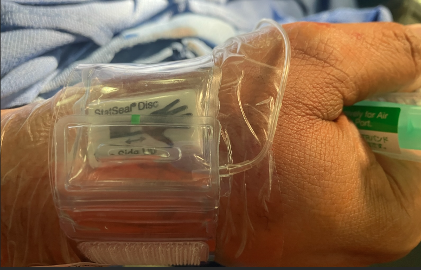
Figure 3B: Distal radial artery access and hemostasis using hemostasis patch.
Related QI Tips
Other evidence-based methods and tools you can use to improve quality of care and outcomes for patients.