Why is the study important?
Aortic stenosis (AS) in females remains underdiagnosed with substantial delays in treatment, surgical or transcatheter. Additionally, females have often represented a minority of subjects enrolled in transcatheter aortic valve replacement (TAVR) trials. Amassing a female-specific evidence base of patients with severe AS is critically important to understanding how to treat these patients effectively.
Should I change my practice because of these findings?
In this pooled analysis from the RHEIA Trial and the PARTNER 3 Trial, female patients with symptomatic severe AS saw higher rates of the composite primary outcome of all-cause death, stroke, or rehospitalization at 1 year when undergoing surgical aortic valve replacement (SAVR) vs. TAVR. Unfortunately, given the relatively young age of patients enrolled in both trials, the question of durability and long-term sustained outcomes remains. In the absence of long-term data, individualized patient-centered and shared decision-making approaches among the Heart Team remains preferred when determining the best therapy for female patients with symptomatic severe AS.
What question was the study supposed to answer?
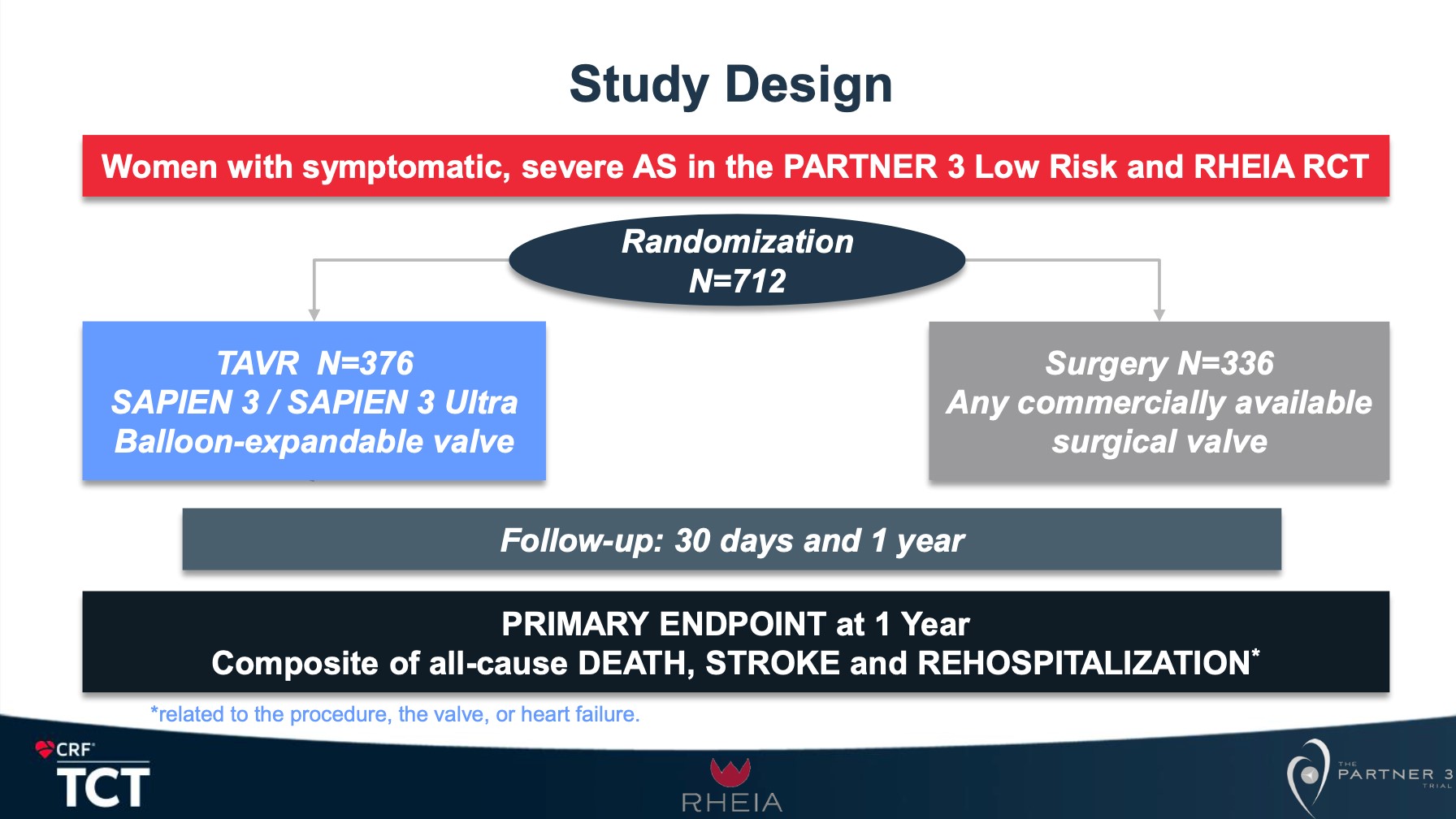
This study sought to compare the 1-year composite of all-cause mortality, stroke, or rehospitalization in patients with symptomatic severe AS randomized to receiving either SAVR or TAVR with a balloon-expandable transcatheter heart valve in either the RHEIA Trial or the PARTER Trial.
What did the study show?
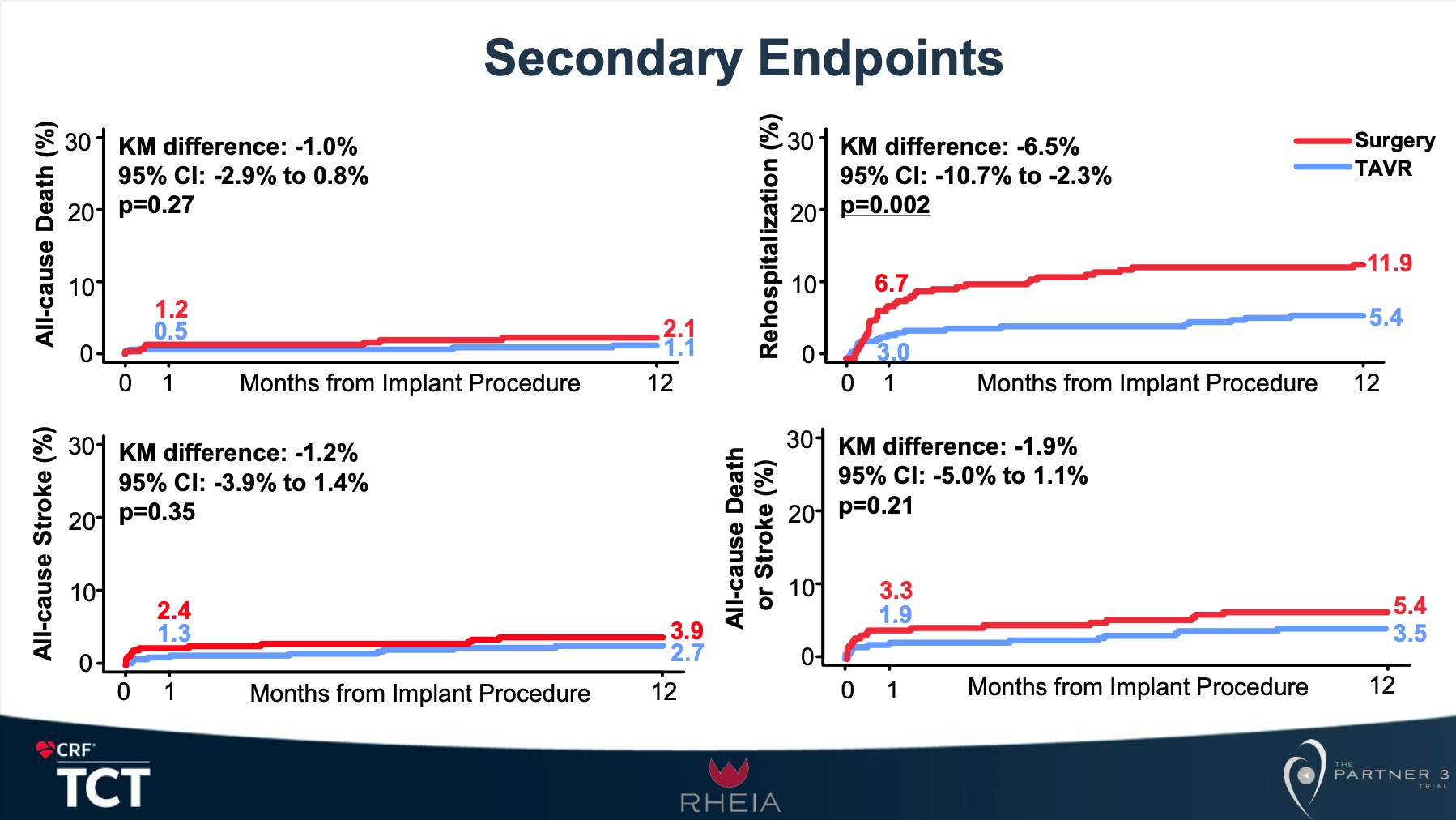
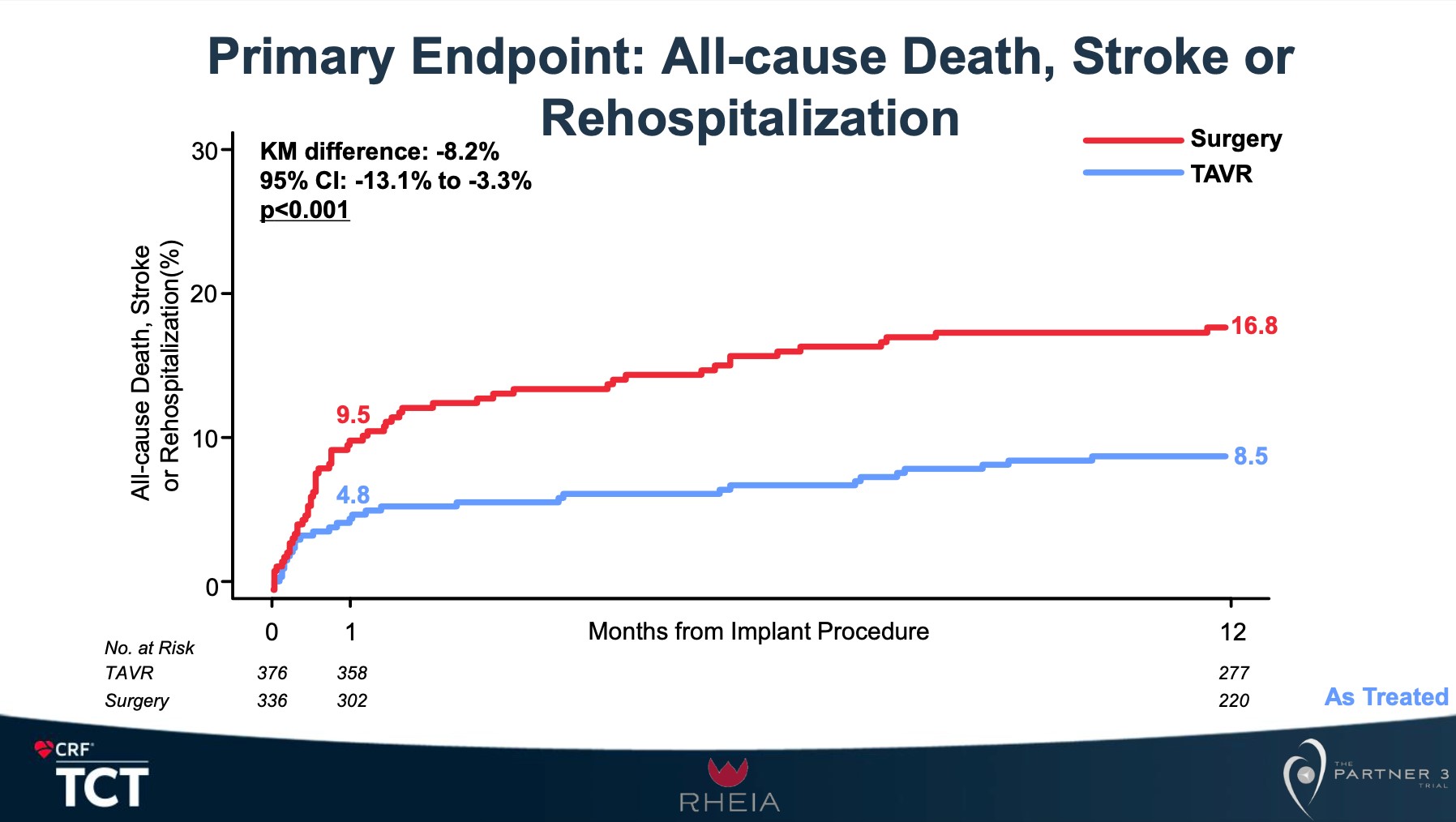
The 1-year analysis of patients enrolled in either the RHEIA Trial or the PARTER Trial compared 376 female subjects who underwent TAVR to 336 subjects who underwent SAVR. Patients had a mean age of 73 years and a mean Society of Thoracic Surgeons score of 2.1%. The mean aortic annular area was 406.7mm2 in the TAVR cohort and 408.7mm2 in the SAVR cohort. The most commonly implanted transcatheter heart valve was a 23mm balloon-expandable valve, and the most commonly implanted surgical valve was either a 21mm or 23mm bioprosthesis. The 1-year composite of all-cause mortality, stroke, or rehospitalization occurred more frequently in those undergoing SAVR compared to TAVR (16.8% vs. 8.5%, p<0.001). This was driven by rates of rehospitalization (11.9% vs. 5.4%, p=0.002). Patients saw higher rates of new-onset atrial fibrillation in the SAVR arm compared to those undergoing TAVR (23.6% vs. 4.0%). Mean gradients following intervention were 2.5mmHg lower in those undergoing SAVR vs. TAVR.
How good was the approach/methodology?
The RHEIA trial was the first multicenter randomized controlled trial comparing exclusively female patients with symptomatic severe AS to either undergoing SAVR or TAVR, demonstrating that in a total of 443 patients, the composite primary composite outcome of all-cause death, stroke, or rehospitalization for valve- or procedure-related symptoms or worsening of heart failure at 1 year occurred more frequently in SAVR compared to TAVR (15.6% vs. 8.9%, p=0.03). The PARTNER 3 Trial was a large multicenter randomized controlled trial comparing patients with symptomatic severe AS deemed to be at low risk for SAVR to TAVR vs. SAVR, demonstrating that at 1-year primary composite outcome of all-cause death, stroke, or rehospitalization was higher in SAVR compared to TAVR (15.1% vs. 8.5%, p=0.001 for superiority). Both trials were leveraged to perform this robust pooled analysis of female subjects. Despite their encouraging short-term findings, long-term data will be needed to clarify durability and lifetime management in these young female patients with symptomatic severe AS.
Other Specialist Resources for Coronary Heart Disease
Including recently published studies, coverage of late-breaking science, updates from clinical trials and registries, and complex case presentations.